Online first
Bieżący numer
Archiwum
O czasopiśmie
Polityka etyki publikacyjnej
System antyplagiatowy
Instrukcje dla Autorów
Instrukcje dla Recenzentów
Rada Redakcyjna
Komitet Redakcyjny
Recenzenci
Wszyscy recenzenci
2025
2024
2023
2022
2021
2020
2019
2018
2017
2016
Kontakt
Bazy indeksacyjne
Klauzula przetwarzania danych osobowych (RODO)
PRACA ORYGINALNA
Umiejscowienie kontroli zdrowia w odniesieniu do aktywności fizycznej i zachowań zdrowotnych wśród studentek pielęgniarstwa: badanie porównawcze dwóch kohort (2016 vs 2026)
1
Independent Researcher, Krakow, Poland
2
Sports Medicine and Human Nutrition, Bronisław Czech Academy of Physical Culture, Krakow, Poland
3
Physical Education and Tourism, Eastern European University of Applied Sciences, Białystok, Poland
4
Department of Foreign Languages, Medical University, Białystok, Poland
5
Nursing, International Academy of Applied Sciences, Łomża, Poland
Autor do korespondencji
Med Og Nauk Zdr. 2026;32(2):134-141

SŁOWA KLUCZOWE
umiejscowienie kontroli zdrowiaaktywność fizycznaIPAQzachowania prozdrowotnestudentki pielęgniarstwa
DZIEDZINY
STRESZCZENIE
Wprowadzenie i cel:
Ocena różnic w samoocenianej aktywności fizycznej, zachowaniach zdrowotnych i umiejscowieniu kontroli zdrowia u studentek pielęgniarstwa oraz analiza powiązań między nimi w dwóch kohortach (2016 i 2026).
Materiał i metody:
Badaniem przekrojowym objęto 473 studentki (2016: N=230; 2026: N=243). Zastosowano Międzynarodowy Kwestionariusz Aktywności Fizycznej (IPAQ), Inwentarz Zachowań Zdrowotnych (IZZ) i Wielowymiarową Skalę Umiejscowienia Kontroli Zdrowia (MHLC).
Wyniki:
Kohorta 2026 wykazała istotnie niższy poziom aktywności fizycznej i zachowań zdrowotnych niż kohorta 2016. Wymiar kontroli zdrowia „Wpływ innych” był w 2026 r. istotnie niższy (p < 0,001), natomiast wymiary „Wewnętrzny” i „Przypadek” nie uległy zmianie. W 2016 r. zachowania zdrowotne korelowały wyłącznie z wymiarem „Wpływ innych” (ρ = 0,18). W 2026 r. korelowały już istotnie z oboma wymiarami: „Wewnętrznym” (ρ = 0,32; p < 0,001) i „Wpływem innych” (ρ = 0,29; p < 0,001). Nie wykazano korelacji między wymiarami MHLC a aktywnością fizyczną w obu grupach.
Wnioski:
Nowsza kohorta przejawia wyższy poziom zachowań sedentarnych, słabsze nawyki prozdrowotne i mniejsze poleganie na autorytetach medycznych. Przejście w 2026 r. do dualnego modelu (gdzie zachowania zdrowotne wiążą się zarówno ze sprawczością wewnętrzną, jak i zewnętrznym wsparciem) podkreśla potrzebę interwencji edukacyjnych łączących samodzielność pacjenta z zaufaniem do profesjonalistów, przy jednoczesnym promowaniu aktywności fizycznej.
Ocena różnic w samoocenianej aktywności fizycznej, zachowaniach zdrowotnych i umiejscowieniu kontroli zdrowia u studentek pielęgniarstwa oraz analiza powiązań między nimi w dwóch kohortach (2016 i 2026).
Materiał i metody:
Badaniem przekrojowym objęto 473 studentki (2016: N=230; 2026: N=243). Zastosowano Międzynarodowy Kwestionariusz Aktywności Fizycznej (IPAQ), Inwentarz Zachowań Zdrowotnych (IZZ) i Wielowymiarową Skalę Umiejscowienia Kontroli Zdrowia (MHLC).
Wyniki:
Kohorta 2026 wykazała istotnie niższy poziom aktywności fizycznej i zachowań zdrowotnych niż kohorta 2016. Wymiar kontroli zdrowia „Wpływ innych” był w 2026 r. istotnie niższy (p < 0,001), natomiast wymiary „Wewnętrzny” i „Przypadek” nie uległy zmianie. W 2016 r. zachowania zdrowotne korelowały wyłącznie z wymiarem „Wpływ innych” (ρ = 0,18). W 2026 r. korelowały już istotnie z oboma wymiarami: „Wewnętrznym” (ρ = 0,32; p < 0,001) i „Wpływem innych” (ρ = 0,29; p < 0,001). Nie wykazano korelacji między wymiarami MHLC a aktywnością fizyczną w obu grupach.
Wnioski:
Nowsza kohorta przejawia wyższy poziom zachowań sedentarnych, słabsze nawyki prozdrowotne i mniejsze poleganie na autorytetach medycznych. Przejście w 2026 r. do dualnego modelu (gdzie zachowania zdrowotne wiążą się zarówno ze sprawczością wewnętrzną, jak i zewnętrznym wsparciem) podkreśla potrzebę interwencji edukacyjnych łączących samodzielność pacjenta z zaufaniem do profesjonalistów, przy jednoczesnym promowaniu aktywności fizycznej.
Introduction and objective:
To evaluate differences in self-reported physical activity, health behaviors, and health locus of control among female nursing students, and to analyze the associations between these variables across two cohorts (2016 and 2026).
Material and methods:
This cross-sectional study included 473 female students (2016: N=230; 2026: N=243). Data were collected using the International Physical Activity Questionnaire (IPAQ), the Health Behavior Inventory (HBI), and the Multidimensional Health Locus of Control (MHLC) scales.
Results:
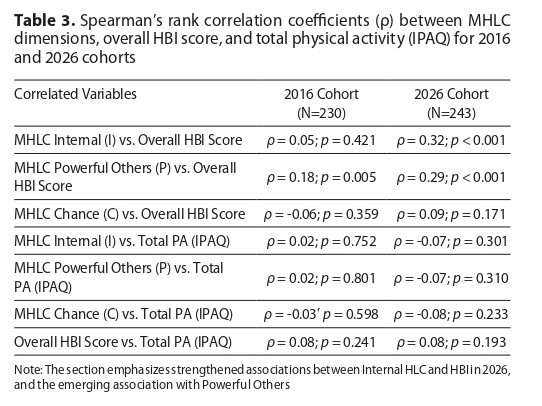
The 2026 cohort demonstrated significantly lower levels of physical activity and health-promoting behaviors compared to the 2016 cohort. The "Powerful Others" locus of control dimension was significantly lower in 2026 (p < 0.001), while the "Internal" and "Chance" dimensions remained unchanged. In 2016, health behaviors correlated exclusively with the "Powerful Others" dimension (ρ = 0.18). In contrast, in 2026, they significantly correlated with both the "Internal" (ρ = 0.32; p < 0.001) and "Powerful Others" (ρ = 0.29; p < 0.001) dimensions. No correlations were found between MHLC dimensions and physical activity in either group.
Conclusions:
The more recent cohort exhibits higher levels of sedentary behavior, poorer health habits, and a decreased reliance on medical authorities. The transition in 2026 to a dual model, where health behaviors are associated with both internal agency and external support, highlights the need for educational interventions that integrate patient autonomy with trust in professionals, alongside the promotion of physical activity.
To evaluate differences in self-reported physical activity, health behaviors, and health locus of control among female nursing students, and to analyze the associations between these variables across two cohorts (2016 and 2026).
Material and methods:
This cross-sectional study included 473 female students (2016: N=230; 2026: N=243). Data were collected using the International Physical Activity Questionnaire (IPAQ), the Health Behavior Inventory (HBI), and the Multidimensional Health Locus of Control (MHLC) scales.
Results:
The 2026 cohort demonstrated significantly lower levels of physical activity and health-promoting behaviors compared to the 2016 cohort. The "Powerful Others" locus of control dimension was significantly lower in 2026 (p < 0.001), while the "Internal" and "Chance" dimensions remained unchanged. In 2016, health behaviors correlated exclusively with the "Powerful Others" dimension (ρ = 0.18). In contrast, in 2026, they significantly correlated with both the "Internal" (ρ = 0.32; p < 0.001) and "Powerful Others" (ρ = 0.29; p < 0.001) dimensions. No correlations were found between MHLC dimensions and physical activity in either group.
Conclusions:
The more recent cohort exhibits higher levels of sedentary behavior, poorer health habits, and a decreased reliance on medical authorities. The transition in 2026 to a dual model, where health behaviors are associated with both internal agency and external support, highlights the need for educational interventions that integrate patient autonomy with trust in professionals, alongside the promotion of physical activity.
Shpakau A, Gacek MK, Sokołowska D, Modzelewski R, Szpakow A. Health locus of control in relation to physical activity and health behaviours
among nursing students – a comparative study of two cohorts (2016 vs 2026). Med Og Nauk Zdr. 2026;32(2):134–141. doi:10.26444/monz/221446
REFERENCJE (26)
1.
World Health Organization. WHO guidelines on physical activity and sedentary behaviour. Geneva, Switzerland: World Health Organization; 2020.
2.
Biernat E, Piątkowska M. Leisure-Time Physical Activity Participation Trends 2014–2018: A Cross-Sectional Study in Poland. Int J Environ Res Public Health. 2019;17(1):208. Published 2019 Dec 27. doi:10.3390/ijerph17010208.
3.
Warburton DER, Bredin SSD. Health benefits of physical activity: a systematic review of current systematic reviews. Curr Opin Cardiol. 2017;32(5):541–556. doi:10.1097/HCO.0000000000000437.
4.
Rogowska AM, Pavlova I, Kuśnierz C, Ochnik D, Bodnar I, Petrytsa P. Does Physical Activity Matter for the Mental Health of University Students during the COVID-19 Pandemic?. J Clin Med. 2020;9(11):3494. Published 2020 Oct 29. doi:10.3390/jcm9113494.
5.
Ciuba A, Kulpa M, Nitsch-Osuch A. The health locus of control and the declared health behavior concerning breast cancer prevention –comparison of Polish women living in urban and rural areas. Ann Agric Environ Med. 2025;32(3):411–417. doi:10.26444/aaem/204854.
6.
Blake H, Stanulewicz N, Mcgill F. Predictors of physical activity and barriers to exercise in nursing and medical students. J Adv Nurs. 2017;73(4):917–929. doi:10.1111/jan.13181.
7.
Mazur J, Dzielska A, Małkowska-Szkutnik A, editors. Zdrowie i zachowania zdrowotne uczniów 17-letnich na tle zmian w drugiej dekadzie życia. Warszawa: Instytut Matki i Dziecka; 2020.
8.
Bergier J, Bergier B, Tsos A. Variations in Physical Activity of Male and Female Students from Different Countries. Iran J Public Health. 2016;45(5):705–707.
9.
Fila-Witecka K, Senczyszyn A, Kołodziejczyk A, et al. Lifestyle Changes among Polish University Students during the COVID-19 Pandemic. Int J Environ Res Public Health. 2021;18(18):9571. Published 2021 Sep 11. doi:10.3390/ijerph18189571.
10.
Duplaga M, Grysztar M. Nutritional Behaviors, Health Literacy, and Health Locus of Control of Secondary Schoolers in Southern Poland: A Cross-Sectional Study. Nutrients. 2021;13(12):4323. Published 2021 Nov 29. doi:10.3390/nu13124323.
11.
Ochnik D, Rogowska AM, Kuśnierz C, et al. Mental health prevalence and predictors among university students in nine countries during the COVID-19 pandemic: a cross-national study. Sci Rep. 2021;11(1):18644. Published 2021 Sep 20. doi:10.1038/s41598-021-97697-3.
12.
Kupcewicz E, Schneider-Matyka D, Rachubińska K, Jastrzębski P, Bentkowska A, Grochans E. Health Behaviours and the Quality of Life of Students of Medical Fields during the COVID-19 Pandemic. Nutrients. 2024;16(11):1747. Published 2024 Jun 2. doi:10.3390/nu16111747.
13.
Marendić M, Aranza D, Aranza I, Vladislavić S, Kolčić I. Differences between Health and Non-Health Science Students in Lifestyle Habits, Perceived Stress and Psychological Well-Being: A Cross-Sectional Study. Nutrients. 2024;16(5):620. Published 2024 Feb 23. doi:10.3390/nu16050620.
14.
Szwamel K, Kowalska W, Mazur E, Janus A, Bonikowska I, Jasik- Pyzdrowska J. Determinants of burnout syndrome among undergraduate nursing students in Poland: a cross-sectional study. BMC Med Educ. 2025;25(1):178. Published 2025 Feb 4. doi:10.1186/s12909-025-06777-9.
15.
Wallston KA, Wallston BS, DeVellis R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Educ Monogr. 1978;6(2):160–170. doi:10.1177/109019817800600107.
16.
Wallston K. Multidimensional Health Locus of Control Scales. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York (NY): Springer; 2013.
17.
Juczyński Z. Narzędzia pomiaru w promocji i psychologii zdrowia. 2nd ed. Warszawa: Pracownia Testów Psychologicznych; 2009.
18.
Luszczynska A, Schwarzer R. Multidimensional health locus of control: comments on the construct and its measurement. J Health Psychol. 2005;10(5):633–642. doi:10.1177/1359105305055307.
19.
Açıkgöz Çepni S, Kitiş Y. Relationship between healthy lifestyle behaviors and health locus of control and health-specific self-efficacy in university students. Jpn J Nurs Sci. 2017;14(3):231–239. doi:10.1111/jjns.12154.
20.
Smoleń E, Dobrowolska B. The health locus of control and chosen health behaviors of nurses from the Lublin and Podkarpackie voivodeships. Nursing Problems / Problemy Pielęgniarstwa. 2018;26(4):290–299. doi:10.5114/ppiel.2018.84129.
21.
Doumit R, Habre M, Cattan R, Abi Kharma J, Davis B. Healthpromoting behaviors and self-efficacy among nursing students in times of uncertainty. Worldviews Evid Based Nurs. 2022;19(6):500–507. doi:10.1111/wvn.12590.
22.
Bácsné Bába É, Lengyel A, Pfau C, et al. Physical activity: the key to life satisfaction – correlations between physical activity, sedentary lifestyle, and life satisfaction among young adults before and after the COVID-19 pandemic. Front Public Health. 2025;13:1486785. Published 2025 Feb doi:10.3389/fpubh.2025.1486785.
23.
Ferreira Silva RM, Mendonça CR, Azevedo VD, Raoof Memon A, Noll PRES, Noll M. Barriers to high school and university students› physical activity: A systematic review. PLoS One. 2022;17(4):e0265913. Published 2022 Apr 4. doi:10.1371/journal.pone.0265913.
24.
Mozafari S, Yang A, Talaei-Khoei J. Health Locus of Control and Medical Behavioral Interventions: Systematic Review and Recommendations. Interact J Med Res. 2024;13:e52287. Published 2024 Oct 10. doi:10.2196/52287.
25.
Nowak PF, Rogowska AM, Kwaśnicka A. The mediating role of health behaviors in the relationship between internal locus of control and life satisfaction in public health students. Sci Rep. 2024;14(1):19112. Published 2024 Aug 17. doi:10.1038/s41598-024-70178-z.
26.
Hendekci A, Koç F. Evaluation of the Peer-Supported E-Health Module Implemented for University Students to Develop Healthy Lifestyle Behaviors. Public Health Nurs. 2025;42(4):1525–1533. doi:10.1111/phn.13563.
Udostępnij
ARTYKUŁ POWIĄZANY
| eISSN: | 2084-4905 |
| ISSN: | 2083-4543 |
Przetwarzamy dane osobowe zbierane podczas odwiedzania serwisu. Realizacja funkcji pozyskiwania informacji o użytkownikach i ich zachowaniu odbywa się poprzez dobrowolnie wprowadzone w formularzach informacje oraz zapisywanie w urządzeniach końcowych plików cookies (tzw. ciasteczka). Dane, w tym pliki cookies, wykorzystywane są w celu realizacji usług, zapewnienia wygodnego korzystania ze strony oraz w celu monitorowania ruchu zgodnie z Polityką prywatności. Dane są także zbierane i przetwarzane przez narzędzie Google Analytics (więcej).
Możesz zmienić ustawienia cookies w swojej przeglądarce. Ograniczenie stosowania plików cookies w konfiguracji przeglądarki może wpłynąć na niektóre funkcjonalności dostępne na stronie.
Możesz zmienić ustawienia cookies w swojej przeglądarce. Ograniczenie stosowania plików cookies w konfiguracji przeglądarki może wpłynąć na niektóre funkcjonalności dostępne na stronie.