CASE REPORT
Impact of physical therapy on the condition of a patient with carpal tunnel syndrome and Raynaud’s disease
1
Higher School of Rehabilitation, Warsaw, Poland
2
Lomza State University of Applied Sciences, Łomża, Poland
3
Eleonora Reicher National Institute of Geriatrics, Rheumatology and Rehabilitation, Warsaw, Poland
Med Og Nauk Zdr. 2021;27(1):82-85

KEYWORDS
TOPICS
ABSTRACT
Introduction:
Carpal tunnel syndrome (CTS) is the most common mononeuropathy that causes median nerve damage at the level of the carpal tunnel. Wrist overload associated with repeated fast movements, often requiring the forced position of the body which loads the wrist joints, is considered to be the most important cause in the formation of CTS. This disease significantly affects patients’ manual skills and limits their daily activities. The use of the best treatment methods can increase the quality of life of CTS people. Correctly performed assessment of the patient’s functional condition allows both the planning, implementation and improvement process, as well as control of the progress of this process. The treatment method for CTS depends on the type, duration and severity of the discomfort. Raynaud’s syndrome is a vasomotor disorder which occurs mostly due to the influence of physicochemical or emotional stimuli. It is observed in 3–15% of the general population, more often among women. The primary character is called Raynaud’s disease, while the secondary is known as Raynaud’s syndrome.
Objective:
The aim of the study was to investigate the effect of classical physical therapy on the condition of a patient with carpal tunnel syndrome and Raynaud’s disease.
Material and Methods:
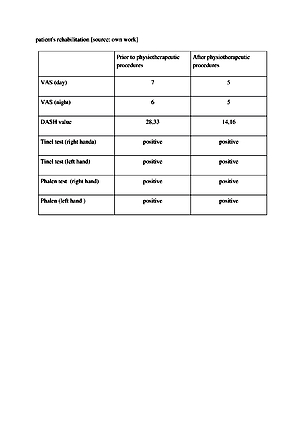
The method of an individual case description was used. The study involved a 36-year-old woman diagnosed with carpal tunnel syndrome and Raynaud’s disease. The material was collected by means of an interview, DASH questionnaire, VAS pain scale and two functional tests: the Phanel and Tinnel tests. Description of the individual case study was based on an interview and physical examination performed before and after rehabilitation.
Results:
Considering the subjective assessment of the achieved improvement after the treatment, the patient noticed a slight decrease in the intensity of pain and numbness, both during the day and at night. The respondent also reported a slight improvement in the function of the upper limbs and improved freedom during some everyday activities.
Conclusions:
Physiotherapeutic procedures slightly reduced the numbness of both the day and night pain. Despite only a few treatments, the patient noticed a slight improvement which confirms that they were correctly selected and should be continued. During the next physiotherapeutic procedure, kinesitherapy should be introduced.
Carpal tunnel syndrome (CTS) is the most common mononeuropathy that causes median nerve damage at the level of the carpal tunnel. Wrist overload associated with repeated fast movements, often requiring the forced position of the body which loads the wrist joints, is considered to be the most important cause in the formation of CTS. This disease significantly affects patients’ manual skills and limits their daily activities. The use of the best treatment methods can increase the quality of life of CTS people. Correctly performed assessment of the patient’s functional condition allows both the planning, implementation and improvement process, as well as control of the progress of this process. The treatment method for CTS depends on the type, duration and severity of the discomfort. Raynaud’s syndrome is a vasomotor disorder which occurs mostly due to the influence of physicochemical or emotional stimuli. It is observed in 3–15% of the general population, more often among women. The primary character is called Raynaud’s disease, while the secondary is known as Raynaud’s syndrome.
Objective:
The aim of the study was to investigate the effect of classical physical therapy on the condition of a patient with carpal tunnel syndrome and Raynaud’s disease.
Material and Methods:
The method of an individual case description was used. The study involved a 36-year-old woman diagnosed with carpal tunnel syndrome and Raynaud’s disease. The material was collected by means of an interview, DASH questionnaire, VAS pain scale and two functional tests: the Phanel and Tinnel tests. Description of the individual case study was based on an interview and physical examination performed before and after rehabilitation.
Results:
Considering the subjective assessment of the achieved improvement after the treatment, the patient noticed a slight decrease in the intensity of pain and numbness, both during the day and at night. The respondent also reported a slight improvement in the function of the upper limbs and improved freedom during some everyday activities.
Conclusions:
Physiotherapeutic procedures slightly reduced the numbness of both the day and night pain. Despite only a few treatments, the patient noticed a slight improvement which confirms that they were correctly selected and should be continued. During the next physiotherapeutic procedure, kinesitherapy should be introduced.
REFERENCES (26)
1.
Oskouei AE, Talebi GA, Shakouri SK, et al. Effects of Neuromobilization Maneuver on Clinical and Electrophysiological Measures of Patients with Carpal Tunnel Syndrome. J Phys Ther Sci. 2014; 26: 1017–1022. https://doi.org/10.1589/jpts.2....
2.
Białoszewski D. Fizjoterapia w ortopedii. Warsaw: PZWL Medical Publishing House; 2014.
3.
Litak J, Grochowski C, Litak J, et al. Carpal Tunnel Syndrome – treatment. J Educ Health Sport. 2017; 7(1): 141–146. http://dx.doi.org/10.5281/zeno....
4.
Ciechanowska K, Łukowicz M. Wpływ sonoterapii na objawy zespołu cieśni kanału nadgarstka. J Educ Health Sport. 2017; 6: 612–616. http://dx.doi.org/10.5281/zeno....
5.
Gniadek M, Trybus M. Zespół kanału nadgarstka – etiologia i leczenie. Prz Lek. 2016; 73(7): 521–530.
6.
Georgiew F, Maciejczak A, Kania A, et al. Ocena przydatności krzywej I/T do diagnostyki zespołu cieśni nadgarstka. Acta Bio-Opt Inf Med Biomed Eng. 2013; 19(1): 40–48.
7.
Gołąbek R, Majcher P. Zespół cieśni nadgarstka. Sport i Turystyka. Środkowoeuropejskie Czasopismo Naukowe 2018; 1(1): 123–140. https://doi.org/10.16926/sit.2....
8.
Nowak M, Jethon J. Zespół kanału nadgarstka – przegląd literatury i doświadczenia własne. Postępy Nauk Med. 2009; 9: 665–672.
9.
Kowalska B, Płaza M. Rola ultrasonografii w diagnostyce neuropatii pourazowych oraz powikłań po operacjach nerwów obwodowych. Pediatr Med Rodz. 2014; 10(3): 265–269.
10.
15557/PiMR.2014.002910. Wilk I. Zastosowanie masażu leczniczego w zespole cieśni kanału nadgarstka. Puls Uczelni. 2015; 9(1): 22–23.
11.
Pasek J, Stanek A, Gębala K, et al. Nowe możliwości balneologii i medycyny fizykalnej u chorych z objawem Raynauda. Acta Balneol. 2015; 2(14 0): 136 –14 0.
12.
Kalużny K, Brola W, Fudala M. Zespół Raynauda w chorobach neurologicznych. Prz Med Uniw Rzesz Inst Leków. 2013; 4: 536–545.
13.
Hartmann P, Mohokum M, Schlattmann P. The association of Raynaud’s syndrome with carpal tunnel syndrome: a meta-analysis. Rheumatol Int. 2012;32: 569–574. https://doi.org/10.1007/s00296....
14.
Wolny T, Linek P. Is manual therapy based on neurodynamic techniques effective in the treatment of carpal tunnel syndrome? A randomized controlled trial Clin. Rehabil. 2019; 33(5): 957–958. doi: 10.1177/0269215518822114.
15.
Mohammadi S, Roostayi MM, Naimi SS, Baghban AA. The effects of cupping therapy as a new approach in the physiotherapeutic management of carpal tunnel syndrome. Physiother Res Int. 2019; 24(3): e1770. https://doi.org/10.1002/pri.17....
16.
Zaralieva A, Georgiev GP, Karabinov V, Iliev A, Aleksiev A. Physical Therapy and Rehabilitation Approaches in Patients with Carpal Tunnel Syndrome. Cureus. 2020; 12(3): e7171. doi: 10.7759/cureus.7171.
17.
Wolny T, Saulicz E, Linek P, Shacklock M, Myśliwiec A. Efficacy of Manual Therapy Including Neurodynamic Techniques for the Treatment of Carpal Tunnel Syndrome: A Randomized Controlled Trial. J Manipulative Physiol Ther. 2017; 40(4): 263–272. doi: 10.1016/j.jmpt.2017.02.004.
18.
Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal Tunnel Syndrome: A Review of Literature. Cureus. 2020; 12(3): e7333. doi: 10.7759/cureus.7333.
19.
Almasi-Doghaee M, Boostani R, Saeedi M, Ebrahimzadeh S, Moghadam-Ahmadi A, Saeedi-Borujeni MJ. Carpal compression, Phalen’s and Tinel’s test: Which one is more suitable for carpal tunnel syndrome? Iran J Neurol. 2016; 15(3): 173–174.
20.
Kuo TT, Lee MR, Liao YY, Chen JP, Hsu YW, Yeh CK. Assessment of Median Nerve Mobility by Ultrasound Dynamic Imaging for Diagnosing Carpal Tunnel Syndrome. PLoS One. 2016; 11(1): e0147051. doi: 10.1371/journal.pone.0147051.
21.
Dakowicz A, Kuryliszyn-Moskal A, Latosiewicz R, et al. Ocena skuteczności dwóch różnych procedur terapeutycznych w leczeniu zachowawczym zespołu cieśni nadgarstka. Reumatolog. 2010; 48(4): 225–229.
22.
Zwolińska J, Kwolek A. Skuteczność leczenia fizjoterapeutycznego pacjentów z zespołem cieśni kanału nadgarstka. Prz Med Uniw Rzesz Inst Leków. 2012; 4: 428–431.
23.
Wilk I. Zastosowanie masażu leczniczego w zespole cieśni kanału nadgarstka. Puls Uczelni. 2015; (9)1: 22–23.
24.
Kocjan J. Efficacy of neural mobilization and mid-carpal mobilization in the treatment of carpal tunnel syndrome. J Educ Health Sport. 2016; 6(6): 31–38.
25.
Ciechanowska K, Łukowicz M. Wpływ sonoterapii na objawy zespołu cieśni kanału nadgarstka. J Educ Health Sport. 2017; 6: 612–616.
26.
Roh YH, Noh JH, Gong HS, Baek GH. Comparative study on the effectiveness of a corticosteroid injection for carpal tunnel syndrome in patients with and without Raynaud’s phenomenon. Bone Joint J. 2017; 99-B(12): 1637–1642. doi: 10.1302/0301- 620X.99B12.BJJ-2017- 0371.R 2.
Share
RELATED ARTICLE
| eISSN: | 2084-4905 |
| ISSN: | 2083-4543 |
We process personal data collected when visiting the website. The function of obtaining information about users and their behavior is carried out by voluntarily entered information in forms and saving cookies in end devices. Data, including cookies, are used to provide services, improve the user experience and to analyze the traffic in accordance with the Privacy policy. Data are also collected and processed by Google Analytics tool (more).
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.